
Significantly prolonged progression-free survival (PFS) and improved response rates were demonstrated in the phase III, MONARCH 3 trial of abemaciclib in combination with the non-steroidal aromatase inhibitors (NSAI), anastrozole or letrozole, in patients with hormone receptor (HR)-positive, HER2-negative advanced breast cancer (ABC).
Angelo Di Leo, Sandro Pitigliani Medical Oncology Department, Nuovo Ospedale di Prato S. Stefano - Istituto Toscano Tumori, in Prato, Italy, presented findings from the phase III, MONARCH 3 trial (NCT02246621) at ESMO 2017, the Annual Congress of the European Society for Medcial Oncology in Madrid, Spain.
An interim analysis done at 194 PFS events showed abemaciclib plus a NSAI significantly prolonged PFS; investigator-assessed median PFS was not reached with the abemaciclib combination compared to 14.7 months with placebo plus a NSAI, hazard ratio (HR) 0.543; 95% confidence interval (CI) 0.409, 0.723 (p = 0.000021).
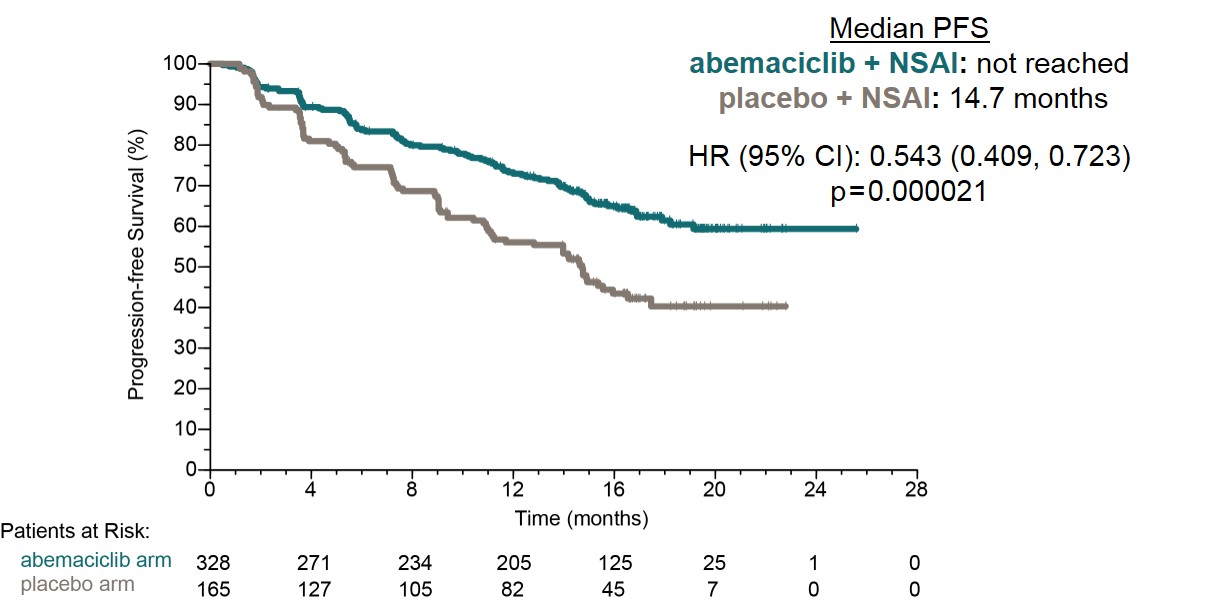
Median PFS.
© Angelo Di Leo.
Anti-tumour activity demonstrated by abemaciclib in patients with measurable disease
MONARCH 3 is a double-blind, phase III study of abemaciclib plus anastrozole or letrozole compared to placebo plus NSAI in postmenopausal women with HR-positive/HER2-negative ABC and no prior systemic therapy in the metastatic setting. Patients were endocrine naive or had progressed greater than 12 months after receiving endocrine therapy. The investigators randomised 493 women 2:1 (328 in the abemaciclib arm, 165 in the placebo arm) who were also stratified according to metastatic site, including visceral, bone only, or other, and by prior endocrine therapy.
Visceral disease was reported in 52.9% of patients, 80.5% had measurable disease, 27.4% of patients had received prior (neo)adjuvant aromatase inhibitors and 39.8% of patients had de novo ABC.
Abemaciclib was administered at 150 mg orally twice daily on a continuous schedule plus either 1 mg anastrozole or 2.5 mg of letrozole, daily.
The primary endpoint for the trial was investigators-assessed PFS and secondary objectives included objective response rate (ORR) and safety. The study was powered to 80% at 1-sided α = 0.025 assuming a HR of 0.67 in favour of abemaciclib plus a NSAI, with analyses at 189 and 240 PFS events.
Patients having measurable disease demonstrated an ORR of 59% with abemaciclib versus 44% with placebo (p = 0.004).
The safety data were generally consistent with results reported in previous trials of abemaciclib. The most common adverse events (AEs) observed were diarrhoea, neutropenia, and fatigue, which occured at rates of 81.3%, 41.3%, and 40.1% with abemaciclib compared to 29.8%, 1.9%, and 31.7% with placebo/NSAI, respectively.
Grade 3 AEs included diarhhoea in 9.5%, and fatigue in 1.8% of patients on abemaciclib and 1.2% of patients on placebo had grade 3 diarrhoea. Grade 3/4 neutropenia was seen in 21.1% of abemaciclib patients versus 1.2% of placebo patients.
Abemaciclib is also being studied in combination with trastuzumab in patients with HR-positive/HER2-positive locally advanced or metastatic breast cancer.
The phase II monarcHER trial (NCT02675231), is assessing abemaciclib plus trastuzumab (with or without fulvestrant) in patients with HR-positive/HER2-positive locally advanced or metastatic breast cancer.
FDA breakthrough designation was granted for abemaciclib, which is a CDK4/6 inhibitor, in 2015 based on a phase I trial wherein single-agent abemaciclib demonstrated an ORR of 31% in 36 patients with heavily pretreated HR-positive breast cancer.1
Conclusions
The authors concluded that abemaciclib combined with a NSAI demonstrated a tolerable safety profile and was an effective initial treatment for patients with HR-positive/HER2-negative ABC that significantly improved PFS and ORR over placebo plus a NSAI.
Nicholas Turner who discussed the study results challenged if the results change standard first line endocrine based therapy. There is a substantial efficacy with safety profile compatible with long term dosing. Consistent benefit across studies reflects the class effect of CDK4/6 inhibitors. No data yet on OS. All CDK4/6 studies are substantially underpowered to look at OS. Median OS on letrozole alone is now approximately 50 months. Realistic power for MONARCH3 is in the range of 50%. There is a clear requirement for collaboration and meta-analysis. In term if these results change whom we give endocrine therapy to, he said yes. He pointed out to one of the main conclusions from the authors, in particular that exploratory subgroup analyses suggest that patients with indicators of poor prognosis had substantial benefit from the addition of abemaciclib, while in some patients with a long treatment-free interval or bone-only disease, single agent endocrine therapy may be an appropriate initial therapy.
Citation
1. Patnaik A, et al. Cancer Discov 2016;6(7):740-53.
Disclosure
This trial was sponsored by Eli Lilly and Company.
Reference
236O_PR - A. Di Leo, et al. MONARCH 3: Abemaciclib as initial therapy for patients with HR+/HER2- advanced breast cancer.